Co-Morbidity of Substance Use
& Mental Health Disorder
A DSM-5 and Scientific Look
at Substance use Disorders
|
|
Treatment for Alcohol & Substance Use Disorders A Training Resource
By Jim Messina, Ph.D., CCMHC, NCC, DCMHS-T
|
|
|
Co-Occurring Disorders of Substance Use & Mental Health Disorders
CEU’s: 3 hours based on request (CE Broker Tracking #: 20-615480)
Resource for Course on Coping.us:
http://www.coping.us/alcoholsubstanceuse/comorbiddisorders.html
Program Description: This program is focused on the co-occurring mental health disorders which can be co-morbid with substance use disorders according to the DSM-5 including: Schizophrenia, Bipolar Disorder, Depression, Anxiety, Obsessive Compulsive Disorder, Sleep-Wake Disorders, Sexual Dysfunctions and Neurocognitive Disorders by the specific substances which have been identified as co-occurring with the specific mental health disorders. There is a need for therapists to understand the brain and neurological functions which lie as the cause of these co-morbidities. There is a need to treat co-occurring disorders in an integrated fashion and not rely on "old school" models of treating them sequentially, parallel separately or left untreated. To help bring home the application of co-morbid interventions case studies will be used widely in this workshop.
Learning Objectives
1.To learn about the tools to assess and Apps to treat these co-morbidities.
2. To learn about the neurological functions in the brain which lie as the cause of these co-morbidities.
3. To learn the rationale behind the need to use integrated treatment strategies when addressing these co-morbidities.
4. To learn about why it is impossible to just treat one condition in isolation from the other co-morbidities if one wants to gain maximal effectiveness for the patients suffering from them.
|
DSM-5's ICD-10-CM Codes for Substance Use Disorders
Specifiers which apply to these disorders where indicated:
- Specify if: In early remission or in sustained remission
- Specify if: In a controlled environment
- Specify if: With perceptual disturbances
Alcohol-Related Disorders
F10.10 Alcohol Use Disorder Mild
F10.20 Alcohol Use Disorder Moderate
F10.20 Alcohol Use Disorder Severe
F10.129 Alcohol Intoxication With use disorder Mild
F10.229 Alcohol Intoxication With use disorder Moderate or severe
F10.929 Alcohol Intoxication Without use disorder
F10.239 Alcohol Withdrawal Without perceptual disturbances
F10.232 Alcohol Withdrawal With perceptual disturbances
F10.99 Unspecified Alcohol-Related Disorder
Cannabis-Related Disorders
F12.10 Cannabis Use Disorder Mild
F12.20 Cannabis Use Disorder Moderate
F12.20 Cannabis Use Disorder Severe
F12.129 Cannabis Intoxication Without perceptual disturbance with use disorder Mild
F10.229 Cannabis Intoxication Without perceptual disturbance With use disorder Moderate or severe
F10.929 Cannabis Intoxication Without perceptual disturbance Without use disorder
F12.122 Cannabis Intoxication With perceptual disturbance with use disorder Mild
F10.222 Cannabis Intoxication With perceptual disturbance With use disorder Moderate or severe F10.922 Cannabis Intoxication With perceptual disturbance Without use disorder
F12.288 Cannabis Withdrawal
F12.99 Unspecified Cannabis-Related Disorders
|
Hallucinogen- Related Disorders
Hallucinogens:
- Indole Alkaloids: ( Lysergic acid diethylamide (LSD); Lysergic acid amide (LSA); Psilocin; Psilocybin)
- Pipendines: (Atropine and scopolamine); Cocaine; Phencyclidine (PCP); Ketamine)
Phenylethylamines:
- (Mescaline, 3,4- methylenedioxymethamphetamine (MDMA), Methylene dioxyamphetamine (MDA), 3-methoxy-4, 5-methylene dioxyamphetamine (MMDA), 3,5-dimethoxy-4-methylamphetamine (STP), 2,5-dimethoxy-4-methylamphetamine (DOM))
Cannabinoids:
- (Delta-9-tetrahydrocannabinol (THC, the active substance in marijuana)
F16.10 Phencyclidine Use Disorder Mild
F16.20 Phencyclidine Use Disorder Moderate
F16.20 Phencyclidine Use Disorder Severe
F16.10 Other Hallucinogen Use Disorder Mild
F16.20 Other Hallucinogen Use Disorder Moderate
F16.20 Other Hallucinogen Use Disorder Severe
F16.129 Phencyclidine Intoxication With use disorder Mild
F16.229 Phencyclidine Intoxication With use disorder Moderate or severe
F16.929 Phencyclidine Intoxication Without use disorder
F16.129 Other Hallucinogen Intoxication With use disorder Mild
F16.229 Other Hallucinogen Intoxication With use disorder Moderate or severe
F16.929 Other Hallucinogen Intoxication Without use disorder
F16.983 Hallucinogen Persisting Perception Disorder
F16.99 Unspecified Phencyclidine-Related Disorder
F16.99 Unspecified Hallucinogen-Related Disorder
|
Inhalant-Related Disorders
Specify the particular inhalant
Mood-altering substances that are voluntarily inhaled
- Butyl nitrite
- Amyl nitrite (Gas in aerosol cans),
- Gasoline and Toluene vapors (Correction fluid, glue, marking pens)
- Most substances used are commercial and household products, such as solvents and aerosols, which are easily obtained and typically not harmful, if used for the purpose intended and as directed
- Because they are common products, inhalants often are a young person’s first attempt at “getting high”
F18.10 Inhalant Use Disorder Mild
F18.20 Inhalant Use Disorder Moderate
F18.20 Inhalant Use Disorder Severe
F18.129 Inhalant Intoxication With use disorder Mild
F18.229 Inhalant Intoxication With use disorder Moderate or severe
F18.929 Inhalant Intoxication Without use disorder
F18.99 Unspecified Inhalant-Related Disorders
|
Opioid-Related Disorders
Opioides:
- Morphine
- Morphine long-acting (Avinza, Kadian)
- HYDROmorphone (Dilaudid)
- OXYcodone (Oxecta): OXYcodone, long-acting (OxyContin)
- HYDROcododone (Vicodin, Lortab) OXYmorphone (Opana)
- OXYmorphone, long-acting (Opana ER)
- Codeine
- Fentanyl
- Methadone
Specify if: on maintenance therapy or in a controlled environment
F11.10 Opioid Use Disorder Mild
F11.20 Opioid Use Disorder Moderate
F11.20 Opioid Use Disorder Severe
F11.129 Opioid Intoxication Without perceptual disturbance with use disorder Mild
F11.229 Opioid Intoxication Without perceptual disturbance With use disorder Moderate or severe
F11.929 Opioid Intoxication Without perceptual disturbance Without use disorder
F11.122 Opioid Intoxication With perceptual disturbance with use disorder Mild
F11.222 Opioid Intoxication With perceptual disturbance With use disorder Moderate or severe
F11.922 Opioid Intoxication With perceptual disturbance Without use disorder
F11.23 Opioid Withdrawal
F11.99 Unspecified Opioid -Related Disorders
|
Sedative-, Hypnotic-, or Anxiolytic-Related Disorders
Sedatives:
Barbiturates:
- Methohexital (Brevital) and thiopental (Pentothal);
- Amobarbital (Amytal), pentobarbital (Nembutal), secobarbital (Seconal), and butalbital (Fioricet, Fiorinal);
- Phenobarbital (Luminal)
Non-Barbiturates:
- Benzodiazepines: Carbamates - Meprobamate (Miltown)
- Chloral derivatives - Chloral hydrate (Noctec) and Ethchlorvynol (Placidyl)
- Piperidines - Glutethimide (Doriden) and methyprylon (Noludar)
- Quinazolinone - Methaqualone (Quaalude)
- Imidazopyridine - Zolpidem (Ambien), zaleplon (Sonata), eszopiclone (Lunesta) and alpidem
- Antihistamines (over-the-counter sleep aids) - Diphenhydramine and doxylamine
- GHB- Gamma-hydroxybutyrate
Hypnotics:
Benzodiazepines:
- Diazepam (Valium, Diastat; Diastat AcuDial)
- Lorazepam (Ativan)
- Midazolam(Versed)
Anxiolytics (Anti-anxiety Meds):
- Alprazolam (Xanax, Niravam, Xanax XR)
- Lorazepam (Ativan)
- Chlordiazepoxide (Librium)
- Clonazepam (Klonopin)
- Clorazepate (Tranxene SD; Tranxene T-Tab)
- Diazepam (Valium, Diastat; Diastat AcuDial)
- Midazolam (Versed)
- Oxazepam (Serax)
F13.10 Sedative, Hypnotic, or Anxiolytic Use Disorder Mild
F13.20 Sedative, Hypnotic, or Anxiolytic Use Disorder Moderate
F13.20 Sedative, Hypnotic, or Anxiolytic Use Disorder Severe
F13.129 Sedative, Hypnotic, or Anxiolytic Intoxication with use disorder Mild
F13.229 Sedative, Hypnotic, or Anxiolytic Intoxication with use disorder Moderate or severe
F13.929 Sedative, Hypnotic, or Anxiolytic Intoxication without use disorder
F13.239 Sedative, Hypnotic, or Anxiolytic Withdrawal Without perceptual disturbance
F13.222 Sedative, Hypnotic, or Anxiolytic Withdrawal With perceptual disturbance
F13.99 Unspecified Sedative-, Hypnotic-, or Anxiolytic- Related Disorder
|
Stimulant-Related Disorder
Amphetamine Related:
F15.10 Amphetamine-Type Substance Use Disorder Mild
F15.20 Amphetamine-Type Substance Use Disorder Moderate
F15.20 Amphetamine-Type Substance Use Disorder Severe
F15.129 Amphetamine or other stimulant Intoxication Without perceptual disturbance with use disorder Mild
F15.229 Amphetamine or other stimulant Intoxication Without perceptual disturbance With use disorder Moderate or severe
F15.929 Amphetamine or other stimulant Intoxication Without perceptual disturbance Without use disorder
F15.122 Amphetamine or other stimulant Intoxication With perceptual disturbance with use disorder Mild
F15.222 Amphetamine or other stimulant Intoxication With perceptual disturbance With use disorder Moderate or severe
F15.922 Amphetamine or other stimulant Intoxication With perceptual disturbance Without use disorder
F15.23 Amphetamine or other substance Withdrawal
F15.99 Unspecified Amphetamine or other substance-Related Disorders
Cocaine Related:
F15.10 Cocaine Use Disorder Mild
F15.20 Cocaine Use Disorder Moderate
F15.20 Cocaine Use Disorder Severe
F14.129 Cocaine Intoxication Without perceptual disturbance with use disorder Mild
F14.229 Cocaine Intoxication Without perceptual disturbance With use disorder Moderate or severe
F14.929 Cocaine Intoxication Without perceptual disturbance Without use disorder
F14.122 Cocaine Intoxication With perceptual disturbance with use disorder Mild
F14.222 Cocaine Intoxication With perceptual disturbance With use disorder Moderate or severe
F15.922 Cocaine Intoxication With perceptual disturbance Without use disorder
F14.23 Cocaine Withdrawal
F14.99 Unspecified Cocaine-Related Disorders
Other or Unspecified Stimulant:
F15.10 Other or unspecified stimulant Use Disorder Mild
F15.20 Other or unspecified stimulant Use Disorder Moderate
F15.20 Other or unspecified stimulant Use Disorder Severe
|
Other (or unknown) Substance-Related Disorders
F19.10 Other (or unknown) Substance Use Disorder Mild
F19.20 Other (or unknown) Substance Use Disorder Moderate
F19.20 Other (or unknown) Substance Use Disorder Severe
F19.129 Other (or unknown) Substance Intoxication With use disorder Mild
F19.229 Other (or unknown) Substance Intoxication With use disorder Moderate or severe
F19.929 Other (or unknown) Substance Intoxication Without use disorder
F19.239 Other (or unknown) Substance
F19.99 Unspecified Other (or unknown) Substance -Related Disorder
|
Co-occurring Substance Use Disorders & Mental Health Disorder Treatment Focus
Substance /Medication – Induced Disorders
- Schizophrenia
- Bipolar Disorder
- Depressive Disorders
- Anxiety Disorders
- Obsessive Compulsive Disorder
- Sleep-Wake Disorders
- Sexual Dysfunctions
- Neurocognitive Disorders
|
|
Case Study #1: Jennifer
My name is Jennifer. I have bipolar disorder and I also have Alcohol Use Disorder. Through over 20 years of being in and out of recovery—and psych wards—and off and on various medications, I have come to realize that I must treat both illnesses in order to recover from either.
I experienced major depressions throughout my young adulthood, making it impossible to hold down a job, show up for friends and family, eat properly, or even bathe regularly. I stayed in bed for weeks at a time. I once took a razor blade and chopped all my hair off. I scratched myself so hard with bitten fingernails that my face was bloody and scabbed. Drinking was the only way to numb the pain. But the manias were even worse, tornadoes racing through my life and the lives of everyone around me. I had multiple psychotic breaks, including a particularly disastrous episode in the south west 16 years ago.
At the time, miserable with a year sober, I concluded that New York was the problem so I moved to a small town in Northern New Mexico. At first it was idyllic—beautiful sun-swept canyons and desert, big crystal blue sky and breathtaking horizons. I was happier than I’d ever been. I drove along gorgeous desert highways with my dog in the back seat, feeling a sense of excitement and joy. I had no idea I was entering the realm of bipolar mania. I just thought I was finally in a good place, after so many episodes of depression.
It really started the afternoon I caught my boyfriend having sex with another girl in my own bed. I walked out of the house, got in my car, and burst into hysterical laughter. Doctors call this type of reaction “inappropriate affect.” I drove all the way to Santa Fe, laughing until my sides hurt, and sat in my car in the Walmart parking lot for several hours, unable to think clearly enough to come up with a plan. Finally, all I could come up with was to return to New York.
Over the next few days, I was torn between my insatiable appetite for sex with that boyfriend (the mania made me hypersexual) and my desperation to get away from him. I repeatedly forgave his indiscretion and then, when he left for his house painting job in the morning, wrote dozens of goodbye letters to him. My little adobe farmhouse was a disaster: boxes half-filled with books and records as I tried to get up the courage to pack the car and leave. The chaos in the house was a physical manifestation of the chaos in my mind. Doctors call this “disorganized thinking.”
One morning I threw a haphazard collection of my stuff in the backseat of my car, along with my dog, my cat, and a puppy I had picked up off the side of the road. I left the house trashed and sped toward Colorado, alternately laughing and crying. I was pulled over near the border for weaving, and the police officer looked concerned when he saw the hodgepodge of junk and animals crammed in the car. I convinced him I was okay, and he let me go—a mistake. Within a few hours I was convinced that the other drivers on the highway were spying on me. I saw dead cows hanging from the telephone poles.
I pulled into a creepy little motel on the edge of a cornfield and locked myself into a room with all my animals milling about. I was convinced the motel desk attendant was spying on me, too. I was afraid to use the phone for fear she would record the conversation, but I knew I needed help so I called my sister in Virginia, who subsequently flew out to Denver to come get me. She later told me how horrible it was to see me huddling in that little room with piles of dog poop all over the place—I was too paranoid to take the animals outside. God bless her, my sister drove me all the way back to New York while I repeatedly threatened to grab the steering wheel and drive into a tree.
After this experience, I was finally put on antipsychotic medication. But I continued to have depressive—and manic—episodes, and I ultimately self-medicated my bipolar disorder with drugs and alcohol. It was not until seven years ago, when I stopped relapsing, got sober and stayed sober, that doctors were able to ascertain exactly what was going on with my brain and prescribe the medication that has saved my life.
As suggested in the AA pamphlet, Medications and Other Drugs, I consulted a doctor who specialized in treating addicts. He took me off the benzos other doctors had wrongly prescribed to me, because those drugs are addictive and I had found it impossible to take them as prescribed. He put me on the non-addictive drug Clozaril, which has kept me stable for seven years. After being hospitalized over a dozen times, I have now managed to stay out of psych wards this entire seven-year stretch. The drug has caused me to gain weight, but I have decided I would rather be stable, sane and overweight than skinny, out of my mind, and hallucinating. Who cares if you are skinny when you are on a locked psych ward?
On the last psych ward I was on, an AA member brought in a meeting for the patients who were dually diagnosed. He proceeded to tell these bipolar and schizophrenic people to stop taking medication that the steps were all we needed.
“If you are depressed, get a new Big Book sponsor and work the steps,” he said. I had been around the block in AA for 15 years, so I knew to ignore this ill advice, but some of the other patients were very confused, and some refused to take their medication that night. The next day, the ward was louder, crazier, and scarier than before, as the non-medicated patients started to spiral into psychosis.
That AA message was dangerous, irresponsible and uninformed, but that AA member was speaking contrary to AA's actual take on the issue. That same AA pamphlet states: “No AA member plays doctor.” It clarifies: “…some members have taken the position that no one in AA should take any medication. While this position has undoubtedly prevented relapses for some, it has meant disaster for others. It is…wrong to deprive any alcoholic of medication which can alleviate or control other disabling physical and/or emotional problems.”
The bottom line is, without sobriety, doctors can’t help me with my bipolar symptoms. But without treating the bipolar disorder, chances are I will drink to self-medicate. No amount of medication will keep me sober, but no amount of step work will keep me from hallucinating dead cows hanging from telephone poles. I must address both issues with equal commitment.
Tentative Diagnosis
Principal Diagnosis
F10.20 Alcohol Use Disorder (severe) in sustained remission (p.490)
F31.74 Bipolar I Disorder Current or most recent episode manic in full remission (p.126)
F10.24 Substance/Medication Induced Bipolar Disorder with Alcohol Use disorder severe (p.142
F19.24 Substance/Medication Induced Bipolar Disorder with unknown substance Use disorder severe (p. 143)
Provisional Diagnosis
None
Other Conditions That May Be a Focus of Clinical Attention
T74-01XA Spouse or Partner Neglect Confirmed Initial Contact (p.721)
T74-31XA Spouse or Partner Abuse, Psychological Confirmed Initial Contact (p.721)
Z65.9 Unspecified Problems Related to Unspecified Psychosocial Circumstances (p.725)
Z91.89 Other Personal Risk Factors (p.726)
Z72.9 Problems Related to Lifestyle (p.726)
Z72.811 Adult Antisocial Behavior (p.726)
Z91.19 Nonadherence to Medical Treatment (p.726)
|
|
What follows are the Classifications for co-occuring Substance use Disorder and Mental Health Disorders
Co-occurring Substance Disorder with Schizophrenic Induced Psychotic Disorder
- Alcohol
- Cannabis
- Phencyclidine
- Hallucinogens
- Inhalants
- Sedatives
- Amphetamines
- Cocaine
Co-occurring Substance Disorder with Bipolar & Related Disorders
- Alcohol
- Phencyclidine
- Hallucinogens
- Sedatives
- Amphetamines
- Cocaine
Co-occurring Substance Disorder with Depressive Disorders
- Alcohol
- Phencyclidine
- Hallucinogens
- Inhalants
- Opioid
- Sedatives
- Amphetamines
- Cocaine
Co-occurring Substance Disorder with Anxiety Disorders
- Alcohol
- Caffeine
- Cannabis
- Phencyclidine
- Hallucinogens
- Inhalant
- Opioid
- Sedative
- Amphetamine
- Cocaine
Co-occurring Substance Disorder with Obsessive-Compulsive Disorder
Co-occurring Substance Disorder with Sleep-Wake Disorders
- Alcohol
- Caffeine
- Cannabis
- Sedative
- Amphetamine
- Cocaine
- Tobacco
Co-occurring Substance Disorder with Sexual Dysfunctions
- Alcohol
- Opioid
- Sedative
- Amphetamine
- Cocaine
Co-occurring Substance Disorder with Delirium & Neurocognitive Disorders
- Alcohol
- Cannabis
- Phencyclidine
- Hallucinogens
- Inhalant
- Opioid
- Sedative
- Amphetamine
- Cocaine
|
Likelihood of SUDs in people with psychiatric diagnoses
Diagnosis Odds Ratio*
Bipolar Disorder 6.6
Schizophrenia 4.6
Panic Disorder 2.9
Major Depression 1.9
Anxiety Disorder 1.7
*Weiss, R.D. & Smith-Connery, H. (2011). Integrated Group Therapy for Bipolar Disorder and Substance Abuse. New York: Guilford Press
|
Why Substance abuse in patients with psychiatric illness?
- Enhanced reinforcement
- Mood Change
- Escape
- Hopelessness
- Poor Judgment
- Inability to appreciate consequences
Results of SUD with Psychiatric Disorder especially Bipolar Disorder
- Lower medication adherence
- Greater chance relapses
- Increased hospitalizations
- Homelessness
- Suicide
Models of Treatment for Dual Diagnosis
- Sequential – Treat SUD first then Psychiatric disorder
- Parallel – Treat both at same time but within different treatment modalities
- Integrated – Treat both at same time within the same treatment modality
Integrated Treatment Model of Treatment of Comorbid Disorders
- Cognitive‐behavioral model focuses on parallels between the disorders in recovery/relapse thoughts and behaviors
- Explores the interaction between the two disorders
- Utilizes a single disorder paradigm: “bipolar substance abuse”
- Uses a “Central Recovery Rule”
Focus of Integrated Model
- Dealing with the Psychiatric disorder without use of Alcohol &/or Drugs
- Confronting denial, ambivalence, acceptance
- Monitoring overall mood during each week
- Emphasis on compliance in taking psychiatric medications
- Identifying and fighting triggers
- Emphasis on “wellness” model of good night’s sleep, balance nutritional intake and exercise
Parallels in Recovery & Relapse thinking between Disorders
- “May as well thinking” vs. “It matters what you do”
- Abstinence violation effect vs. stopping taking psychiatric meds when anxious or depressed
- Recovery thinking vs. relapse thinking and acting out
- Remember: you’re always on the road to getting better or getting worse: “It matters what you do!”
The Central Recovery Rule
No matter what
- Don’t drink
- Don’t use drugs
- Take your medication as prescribed
No matter what
Weiss, R.D. & Smith-Connery, H. (2011). Integrated Group Therapy for Bipolar Disorder and Substance Abuse. New York: Guilford Press.
|
|
CASE Study 2: Alexia
Last week, Alexia entered an inpatient treatment program. She is being treated for alcohol and cocaine (crack) dependence. Alexia is a 32-year-old, divorced woman who is employed as an administrative assistant at a local human services program. She lives with her 11-year-old daughter, Christine, in an apartment located near her job. Although she makes a relatively low salary, Alexia has managed to support herself and her daughter without financial support from Christine's father. Alexia was married briefly to Christine's father when she was 20, but she left him after he became physically and sexually abusive toward her. He also was an alcoholic. She had almost no contact with him for many years. Her mother, a widow, is a strong support for Alexia and Christine, as are two cousins, Denise and Moira. Alexia reports growing up in a "normal middle class family" and states that her childhood was "good" despite her father's occasional drinking binges, which she says were related to him celebrating a special account he had landed (he was in advertising), and her mother's "occasional bad depressions." She is the youngest of five children and the only girl.
Up until a month ago, Alexia was regularly attending twice-weekly treatment sessions at an outpatient chemical dependency clinic, and she went to AA/NA regularly 3 times a week. She had a sponsor and they kept in touch several times a week or more, if needed. From the beginning of recovery, Alexia has experienced some mild depression. She describes having little pleasure in life and feeling tired and "dragging" all of the time. Alexia reports that her difficulty in standing up for herself with her boss at work is a constant stressor. She persisted with treatment and AA/NA, but has seen no major improvement in how she feels.
After Alexia had been sober for about 3 months, an older boy sexually assaulted Christine after school. Alexia supported Christine through the prosecution process; the case was tried in juvenile court and the boy returned to school 2 months later.
After Alexia celebrated her 6-month sobriety anniversary, she reports that she started having a harder time getting herself up each day. Around this same time, she returned to drinking daily. She says that she then started experiencing bouts of feeling worthless, sad, guilty, hopeless, and very anxious. Her sleep problems increased, she began having nightmares, and she lost her appetite. After a month of this, she started attending AA/NA and treatment less often, instead staying home and watching TV. She started her crack use again one night after her boss got very upset with her not finishing something on time. She went to a local bar after work that day and hooked up with a guy she met there to get crack. In accompanying him to a local dealer's house to get some crack, she was raped by several men. Alexia did not return home that night (Christine was at a friend's sleepover party) and did not show up for work the next day. She does not recall where she was the rest of that night. However, later that day she admitted herself to the treatment program.
Alexia reports that she began drinking regularly (several times a week) around the age of 13. She recalls having felt depressed around the same time that she began drinking heavily, although she states she has very few clear memories of that time in her life. Alexia's drinking became progressively worse over the years, although she did not begin to see it as a problem until after she began using crack, at around age 28. She reports feeling depressed over much of her adult life, however her depression got much worse after she began using crack daily.
Alexia reports having had a lot of gynecological problems during her 20s, resulting in a hysterectomy at age 27. When asked if she was ever physically or sexually abused as a child, she says no; however, she confesses (with some difficulty) that when she was 11, she had an affair with her 35-year-old uncle (father's brother-in-law).
Now, one week into treatment, Alexia reports feeling numb and tense. She talks only in women's treatment groups and, then, only when specifically asked a question. She feels hopeless about her ability to put her life together and says that she only sees herself failing again to achieve sobriety. Of her recent rape, she says that she "only got what she deserved" for being in the wrong place with the wrong people at the wrong time. Alexia reflects that she was unable to adequately protect her daughter from sexual assault, and she speculates that maybe she is an unfit mother and should give up custody of her daughter. While Christine is currently staying with Alexia's mother, Alexia is concerned that her ex-husband will try to get custody of Christine if he hears that she is in the hospital for alcohol and drug treatment. He has been in recovery himself for two years and began demanding to see Christine again about 2 months ago.
Tentative Diagnosis
Principal Diagnosis
F43.10 Posttraumatic Stress Disorder (p.271)
F33.2 Major Depressive Disorder, Recurrent Episode (Severe) (p.162)
F14.20 Stimulant Related Disorder, Crack Cocaine (p.562)
F10.20 Alcohol Use Disorder (severe) (p.490)
Provisional Diagnosis
F10.282 Medication-Induced Sleep Disorder, Alcohol, (Severe) (p.415)
F14.282 Medication-Induced Sleep Disorder, Cocaine, (Severe) (p.417)
Other Conditions That May Be a Focus of Clinical Attention
Z62.820 Parent Child Relational Problems (p.715)
Z63.0 Relationship Distress with Spouse or Intimate Partner (p.716)
Z63.8 High Expressed Emotion Level Within Family (p.716)
T74.22XA Child Sexual Abuse, Confirmed, Initial encounter (p.718)
Z62.810 Personal History (Past History) of sexual abuse in childhood (p.718)
T76.32XA Child Psychological Abuse, Suspected, Initial encounter (p.719)
Z91.410 Personal History (Past History) of Spouse or Partner Violence, Physical (p.720)
T74.21XA Spouse or Partner Violence, Sexual, Confirmed, Initial encounter (p.720)
9T76.31XA Spouse or Partner Abuse, Psychological, Suspected, Initial encounter (p.721)
T74.21XA Adult Sexual Abuse by Non-Spouse or Non-Partner, Confirmed, Initial encounter (p.722)
Z56.9 Other Problem Related to Employment (p.723)
Z59.6 Low Income (p.724)
Z65.4 Victim of Crime (p.725)
Z91.49 Other Personal History of Psychological Trauma (p.726)
Z72.9 Problem Related to Lifestyle (p.726)
Z90.710 Personal History of surgery to other organs (Vaginal Hysterectomy)
|
|
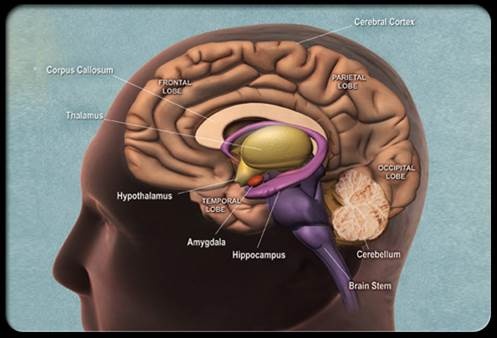
Neuroscience Look at Substance Use Disorders
Frontal (Executive) Cortical Function
- Focus attention
- Prioritize
- Exclude extraneous information
- Suppress primitive urges
- Reduce impulsivity
Non-Addict Response
“This is dangerous”
Prefrontal cortex
- Sends inhibitory signals to the Ventral Tegmental Area (VTA)
- Reduces dopamine release
No repetitive use pattern
No reinforcement of pleasure
Addict Response Pattern
“Got to have more”
Cognitive Deficit Model
Abnormalities in prefrontal cortex
- Compromised ability to send inhibitory signal to VTA
- Chronic alcoholics have reduced GABA
Neurochemical used in the inhibitory process
- Meth and Coke may damage this brain loop
- Frontostriatal loop
|
|
Case Study 3: Robbie
Robbie J., a 19-year-old white male and first-year college student, suffered a significant brain injury 6 months ago as a result of a car accident. Robbie had been partying at a friend's house and left about 1:00 a. m. Driving home, he missed a curve in the road and rolled his car. Robbie's parents knew that their son drank "occasionally," but they never thought he had a "problem." They had purchased a car for him and warned him of the dangers of drinking and driving.
Prior to the accident, Robbie had been a gregarious young man. In high school he had been a good student, popular, and played on the football team. Robbie loved skiing, skin diving, and riding dirt bikes. Robbie's rehabilitation has been arduous. His parents are still in disbelief. Robbie's father is a prominent corporate attorney, and Robbie had always expressed a desire to follow the same career path. Robbie's mother divided her time between caring for her husband and son and her volunteer work on behalf of abused and neglected children in the community. Since his injury, Robbie's mother has spent most of her time caring for him and participating in his rehabilitation. His father is spending longer hours at work and misses the time he spent hunting, fishing, and playing golf with his son. Though supportive at first, his friends are calling less and less and rarely come around.
Both parents were stunned to learn that Robbie and some of his friends got drunk nearly every weekend. This information surfaced during a family counseling session conducted by a counselor on the rehabilitation team who had recently attended a seminar on screening and brief intervention for alcohol and other drug problems. Robbie's parents had a hard time believing it was true, but after questioning Robbie's friends, they learned that this was indeed the situation.
The brain damage Robert sustained has affected his impulse control and decreased his short-term memory and ability to concentrate. Robbie's emotional affect is labile. At times he laughs out loud; the next moment he may be crying. He has limited insight into his own behavior and how he has changed, so it is difficult for him to understand why his friends and family react to him differently now. Very few things sustain Robbie's attention; even watching TV is not pleasurable. The muscle weakness on his right side limits his ability to participate in many of the athletic activities he enjoyed previously.
Robbie is on an emotional roller coaster. At one level he knows that his plans for the future have to change. At another level, he cannot accept these limitations. He wants things to be the way they were. His condition makes it impossible for him to return to a successful college experience. He resents his parents' constant supervision, and feels that they are "treating him like a baby." He says no girl will want to date him with this kind of interference. Most of his friends are back at college, so he has begun to hang out with a younger group and drink again. Robbie is frustrated with the difficulty he has in remembering, expressing himself, and concentrating. He is restless and agitated sometimes, both as a result of his frustration and the organic aspect of his injuries. Robbie's parents can afford high quality treatment, but Robbie does not always comply with the treatment regimen.
Tentative Diagnosis
Principal Diagnosis
S06.2X9S diffuse traumatic brain injury with loss of consciousness of unspecified duration, sequela (p.624)
F02.81 major neurocognitive disorder due to traumatic brain injury, with behavioral disturbance (p.624)
F10.10 Alcohol use disorder, mild (p.490)
F43.20 Adjustment disorder, with mixed disturbance of emotions and conduct (p.286)
Provisional Diagnosis
S06.2X9S diffuse traumatic brain injury with loss of consciousness of unspecified duration, sequela (p.624)
F06.31 Depressive disorder due to another medical condition, with depressive features (p.180)
Other Conditions That May Be a Focus of Clinical Attention
Z62.820 Parent-Child Relational Problem (p.715)
Z63.8 High Expressed Emotion Level Within Family (p.716)
T76.02XA Child neglect, suspected, Initial encounter (p.717)
Z55.9 Academic or Educational Problem (p.723)
Z60.0 Phase of Life Problem (p.724)
Z60.4 Social Exclusion or Rejection (p.724)
Z91.19 Nonadherence to Medical Treatment (p.726)
|
|
Driving Forces of Addictive Disorder
- Acute Abstinence Syndrome
- Situational and emotional triggers
- Reward and reinforcement
Tolerance
Brain cells gradually become less responsive
- More is needed to stimulate the VTA brain cells
- To cause more release of dopamine in the NAc
- To produce reward comparable to earlier experiences
Acute Abstinence Syndrome (Heroin)
Locus Coeruleus (LC)
Norepinephrine (NE)
- Wakefulness
- Breathing
- Blood pressure
- General Alertness
Heroin attaches to mu opioid receptors in LC
- Suppression of NE
- Drowsiness
- Slowed respiration
- Low blood pressure
Symptoms of the Abstinence Syndrome (Heroin)
Addicts experience- A hyper-aroused state(“fight or flight”) with
Increased :
- Heart rate
- Blood pressure
- Restlessness
- Tremors
- Hypervigilence
- Dilated pupils
Symptoms of the Abstinence Syndrome (Heroin)
Addicts experience-worst case of flu imaginable
- Nausea and vomiting
- Runny nose
- Cold,shivering
- Cramping
- Tearing
- Diarrhea
Multiple Interlocking Neurotransmitter Systems
Dopaminergic system
Serotonergic system
Noradrenergic system
Gamma amino butyric acid (GABA) system
Glutamatergic system
Acute Abstinence Syndrome
Mesolimbic Reward System
- Reduction of the VTA’s release of dopamine into Nucleus Accubens (NAc) resulting in Anhedonia
Changes in reward system are part of craving and compulsive drug use
Principles of Acute Management
- Long acting for short acting
- Intoxication not necessary
- 20-30% reduction will not precipitate an abstinence syndrome
- Long term slow withdrawal without patients knowledge of dosage best in outpatient
Alcohol Acute Abstinence Syndrome
- Activation of excitatory glutamatergic system which can induce-Seizures
- Inhibition of inhibitory GABA system
- Net effect is sympathetic nervous system hyperactivity
Medication Management of Alcohol Acute Abstinence Syndrome
Benzodiazepines
GABA agonists
- Attenuate GABA activity
- Reduce seizure risks
Long acting benzodiazepines
- Chlordiazepoxide (Librium)
- Diazepam (Valium)
- Clonazepam (Klonopin)
Alpha-2 Adrenergic Agonists-Reduce Norepinephrine activity
- Clonidine (Catapres)
- Lofexidine (Britlofex)
Beta-Adrenergic Blockers-Block peripheral symptoms
- Tremors
- Increased heart rate
- Sweating
- Propranolol (Inderal)
Medications To Reduce Alcohol Relapse Rate
Disulfiram (Antabuse)
- Inhibits liver enzyme aldehyde dehydrogenase
Revia (Naltrexone)
- Opioid antagonist
- Enhanced release of Beta-Endorphins with family history
Acamprosate
- Inhibits Glutamatergic activity
- Enhances GABA activity
Selective Serotonin Reuptake Inhibitors-Reduce amount of drinking in heavy drinkers
- Fluoxetine (Prozac)
- Citalopram (Celexa)
Topiramate (Topamax)
- Enhances GABA functioning
- Decreases Glutamatergic functioning
- Cognitive (concentration) problems
Situational and Emotional Triggers
Personality and change
Therapy/symptom match
Motivation
Psychotherapy
- Cognitive Therapy
- Behavior Therapy
Cognitive dysfunction and change
Education
Personality and Change
- Temperament
- Character
- Introvert vs. Extrovert
- Personality Disorder
- Cognitively open vs. closed
- Degree of impulsivity
- Stimulus seeking
Therapy/Symptom Match
Matching therapy to symptoms
- Cognitive-pessimism and self doubt, negative “self-talk”, “stinking thinking”
- Pharmacological-moderate to severe symptoms
- Interpersonal-social isolation and disturbed relationships
- Family/Couples-domestic conflict
- Insight-guilt, anger and emotional turmoil
- Behavioral-negative behaviors
- Motivational-no plans or ambivalence to change
All treatments ultimately affect all symptoms
Symptoms are related
Therapist must find a place to break into the circle
Motivation
- Motivational Interviewing
- Motivational Enhancement Therapy
- Evoking self-motivation
- Asking open-ended questions
- Stages of change model
Evoking Self-Motivation
Questions to ask
- What things make you think that this is a problem?
- What do you think will happen if you do not make a change?
- What are the reasons you see for making a change?
- What makes you think you need to make a change?
- What makes you think that if you decided to make a change, you could do it?
- What do you think would work for you, if you needed to change?
- How much does your use concern you?
Open-Ended Questions
What brings you here today?
- So you are here to talk about quitting.
In what ways are you concerned about your marijuana use?
- Do you use marijuana too much?
What do you think you want to do about your use?
- When do you plan to quit?
Stages of Change Model
- Precontemplation
- Contemplation
- Preparation
- Action
- Maintenance
Precontemplation
Task- to increase discrepancy
Educational confrontation
- How many joints do you smoke?
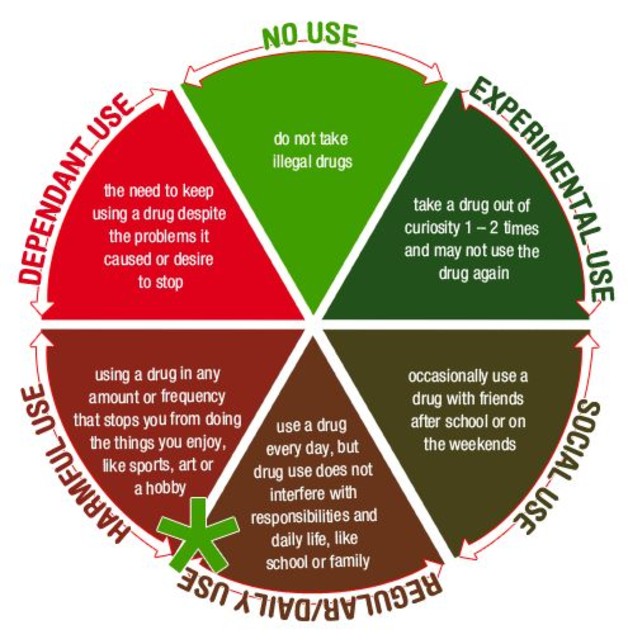
- Use progression models
- Accurate information about disease
- Educational model
Good and less good aspects
- Good and bad aspects
- Invites defensiveness
- Narcissistic defense
Broad based assessment
- Alcohol and drug history
- Psychosocial history
- Psychiatric evaluation
- Medical evaluation
Contemplation
Task- tip the decisional balance scale
Normalize ambivalence
- I know many other clients who felt the same way as you and they succeeded.
- You are the best judge of which way to go.
- Use reframes
What are the options?
- Move from external to internal motivation
- Real from perceived
There are many problems
- Deal with first other issue
- “Natural link”
Quit drinking for a week
Take meds for a month
List of concerns
Questions
- It’s up to you…….
- What do you plan to do next?
- What is most important reason to change?
- Where do we go from here?
- How would you like for things to turn out?
Psychotherapy
Behavior Therapy
- Understand and Change Negative Behaviors
- Positive Reinforcing Behaviors
New Social Environment
New Friends
New Activities
Based on ego-strength or level of developmental maturity
- Problem solving
- Experiential role-play
- PPT group
Contingency management
Cognitive Behavioral Therapy
Cognitive Therapy Automatic Thoughts
- “I cannot do anything right”
- “I fail at everything I do”
- “I will never get better”
- “No one can help me”
- “No one understands me”
Develop a Dynsfunctional Thought Record
Automatic Thought - Emotion - Alternative Response - Result
Cognitive Dysfunction and Change
Frontal cortex vs. midbrain
Approximately 50% entering treatment suffer from cerebral (cognitive) dysfunction
- Less likely to attend continuing care
- Less likely to be employed
- Often mistaken as resistant or unmotivated
- Less able to absorb information
Stimulant addicts look like they have degenerative brain disease
Executive and visuospatial functioning problems include:
- Recent memory
- Abstraction
- Problem solving
- Cognitive flexibility
- Planning
- Rapid Response
Recovery in neuropsychological functioning - Most of treatment is during time of greatest dysfunction
Recovery is:
- Time-dependent
- Due to sustained abstinence
- Experience-dependent
- Active rehabilitation or repetitive behavior
Education
Why give a cocaine or methamphetamine addict a 60 minute didactic or video?
A new format
- 15-20 minute simple didactic - How to participate in treatment
- 10 minute questionnaire
- 30 minute discussion group
10 Minute Questionnaire
I think...
I feel...
I learned...
My future behavior will change in this way....
Reward and Reinforcement
- Mesolimbic Reward Center
- Allostasis and Anhedonia
- Environment
- Spirituality
Mesolimbic Reward System
- Drug enters the system (heroin)
- Attaches to specialized protein - Mu opioid receptor
- Activates Ventral Tegmental Area (VTA)
- Nucleus Accumbens (NAc) releases dopamine
- Pleasure (reward)
Reward and Reinforcement
Three-way link
- Environment
- Dopamine D2 Receptor function
- Drug self-administration
Allostasis and Anhedonia
6-7 second “mental orgasm”
What’s in it for me?
Allostasis
- Inability to return to previous homeostatic levels
Anhedonia
- Inability to experience pleasure
Allostasis
- Addictive drugs dysregulate the brains reward center
- Brain stabilizes at a more negative affect state
- “Normal” becomes a more negative and unpleasant reality
- “Use just to feel normal”
Anhedonia
Attributed to a lowered level of dopamine
Cocaine and methamphetamine
Selegiline (Carbex, Atapryl)
- MAOI
- Believed to restore depleted dopamine
Modafinil (Provigil)
- Treatment for Narcolepsy
- Increases mood, energy, and sense of well-being
- Reduces daytime sleepiness
Heroin
Methadone
Clonidine
Environment
- Triggers or cues (seeing, smelling, touching, tasting, and hearing)
- that remind the addict of some aspect of his/her use
- increase the desire for the reward (craving) without necessarily enhancing the pleasure of the reward itself.
- Living in an enriched environment may reduce animals self-administration of drugs
- Animal studies suggest that environmental conditions may affect the activity of dopamine
Impact the The Environment through
Case Management
Multisystem Therapy
“Wrap around” services
- Family and childcare services
- Housing/Transportation services
- Financial and legal services
- AIDS and medical services
- Addiction and mental health services
- Vocational and educational services
|
|
Case Study 4: Ms Cook
Ms. Cook is a 28-year-old African American woman who voluntarily approached the primary provider agencies for substance abuse treatment services. She is currently on probation for shoplifting, passing bad checks, vandalism, and parole/probation violations. She has been charged four times with disorderly conduct, once for fishing without a license, and twice for driving without a license (she never applied for one). She is currently awaiting trial for battery. Ms. Cook has been incarcerated twice during her adulthood (once for 10 months and, most recently, for 10 days).
The results of an AUDIT-13 screening suggested that she was binge drinking weekly during the past year. The screening also determined that, because of drinking/drug use, she had injured herself (2 falls requiring medical care) and someone else (killed the cat by accidental poisoning), and that others had recommended that she seek help.
Screening for co-occurring problems using the MPSI-A indicated potential depression and other psychological distress. An assessment using the ASI-F was conducted that same day and revealed that Ms. Cook was currently living with her grandmother, who had raised her. She is the mother of four children (ages 11, 7, 4, 2 years-she was 17 at the birth of her first child). The older two sons are living in foster care. The younger two daughters have complex health problems and developmental delays; they live with another relative. She is no longer in contact with any of the children's fathers (three men), and was only briefly married to the second man. She reported that both of her parents, several uncles and aunts, and both of her siblings all have significant drinking and/or drug use problems. She has no close friends and a distant, conflicted relationship with family members other than the grandmother with whom she has almost always lived. She has great difficulty in "getting along" with people. She was physically abused as a child, which prompted her move to the grandmother's home. Ms. Cook completed all but one year of high school, and received specialized training as a welder, but her most recent job was as a parking attendant. Her longest period of continuous employment was just over one year, and she has worked irregularly throughout her adult life. She describes her present health as "good" and she has a history of depression, anxiety, hallucinations, cognitive and memory deficits, and violent behavior. She has never received psychiatric care.
Ms. Cook identified her primary problem as alcohol use, along with regular marijuana (smoking and eating). She began drinking at age 14 and using marijuana at age 17; she began using crack cocaine from the time she was 22. She has been detoxed on three separate occasions. The longest that she has gone without using any substances was 60 days; she resumed using approximately two months ago. Ms. Cook reported that she was extremely troubled and concerned about her substance use and that seeking treatment is very important to her.
Tentative Diagnosis
Principal Diagnosis
F60.2 Antisocial Personality Disorder (p.659)
F10.20 Alcohol Use Disorder Severe (p. 490)
F12.20 Cannabis Use Disorder Severe (p. 509)
F14.20 Cocaine (Crack) Use Disorder Severe (p.562)
Provisional Diagnosis
F10.24 Substance/Medication induced Depressive Disorder with Alcohol use disorder Moderate (p.175)
F14.24 Substance/Medication induced Depressive Disorder with Cocaine use disorder Moderate (p.175)
F10.280 Substance/Medication Induced Anxiety Disorder with Alcohol Use disorder Moderate (p.226)
F12.280 Substance/Medication Induced Anxiety Disorder with Cannabis Use disorder Moderate (p.226)
F10.24 Substance/Medication Induced Bipolar Disorder with Alcohol Use disorder moderate (p.142)
F43.8 Other Specified Trauma- and Stressor-Related Disorder Adjustment-like disorder with prolonged duration of more than 6 months without prolonged duration of stressor (physical abuse) (p.290)
Other Conditions That May Be a Focus of Clinical Attention
Z62.820 Parent-child relational problem (p.715)
Z62.891 Sibling relational problem (p.715)
Z62.29 Upbringing away from parents (p.716)
Z62.898 Child affected by parental relationship distress (p.716)
Z63.0 Relationship distress with spouse or intimate partner (p.716)
Z63.5 Disruption of family by separation or divorce (p.716)
Z63.8 High expressed emotion level within family (p.716)
Z62.896 Uncomplicated bereavement (p.716)
T74-12XA Child Physical Abuse Confirmed Initial Contact (p.717)
Z69.810 Personal history (past history) of physical abuse in childhood (p.718)
Z55.9 Academic or Educational Problems (p.723)
Z56.9 Other Problem Related to Employment (p.723)
Z59.9 Unspecified Housing or Economic Problems (p.724)
Z60.3 Acculturation Difficulty (p.724)
Z60.4 Social Exclusion or Rejection (p.724)
Z60.5 Target of (Perceived) Adverse Discrimination or Persecution (p.724)
Z60.9 Unspecified Problem Related to Social Environment (p.725)
Z65.0 Conviction in Civil or Criminal Proceedings Without Imprisonment (p.725)
Z65.1 Imprisonment or Other Incarceration (p.725)
Z65.2 Problems Related to Release from Prison (p. 725
Z65.2 Problems Related to Other Legal Circumstance (p.725)
Z64.1 Problems Related to Multiparity (Parent having many children) (p. 725)
Z64.4 Discord with Social Service Provider, Including Probation Officer, Case Manager, or Social Services Worker (p.725)
Z65.9 Unspecified Problems Related to Unspecified Psychosocial Circumstances (p.725)
|
|
|
|