Behavioral Medicine's Evidence Based Practices
|
|
Behavioral Medicine for Mental Health Professionals
A Training Resource
By Jim Messina, Ph.D., CCMHC, NCC, DCMHS-T
|
|
|
Importance of Evidence Based Practices within Medical Setting
Therapists within an Integrated Medical Team are officially referred to as Behavioral Health Consultants (BCH’s) and they are expected to bring their EBP’s for the mental health disorders which the Medical team will encounter.
The embracing of Evidence Based Practices (EBP’s) within Integrated Medical Settings has major importance on how effectively and efficiently Behavioral Health Consultants (BHC’s) provide services to their patients within an accountable and sound ethical model.
|
Why use Evidence Based Practices within a Medical Setting?
Reality is that all physicians, nurses, rehabilitation therapists and other hands-on medical interventionists utilize ONLY Evidence Based Medical Treatments with proven effectiveness when treating patients. This is what is meant by the medical Model
The Medical Model involves:
1.Identifying the Target Medical Condition the Patient has brought to the table
2.Identifying the Evidence Based Treatment which has a proven track record in the treating of this medical condition
3.Following the rubric of the Evidence Based Treatment to ensure accuracy and accountability with both the patient and the Medical Organizations treating the patient
|
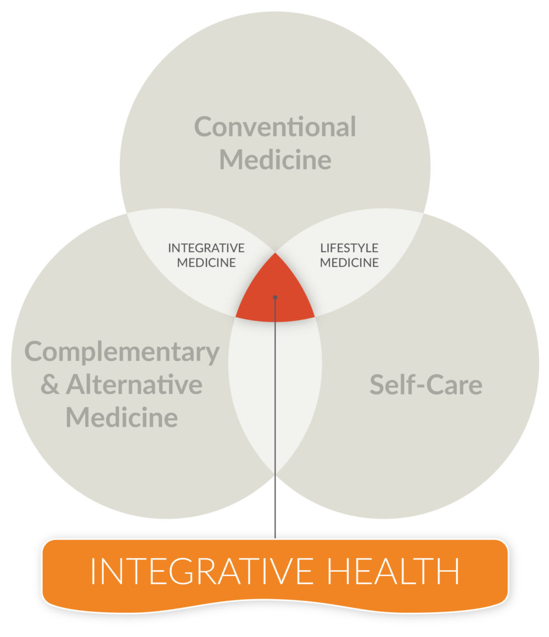
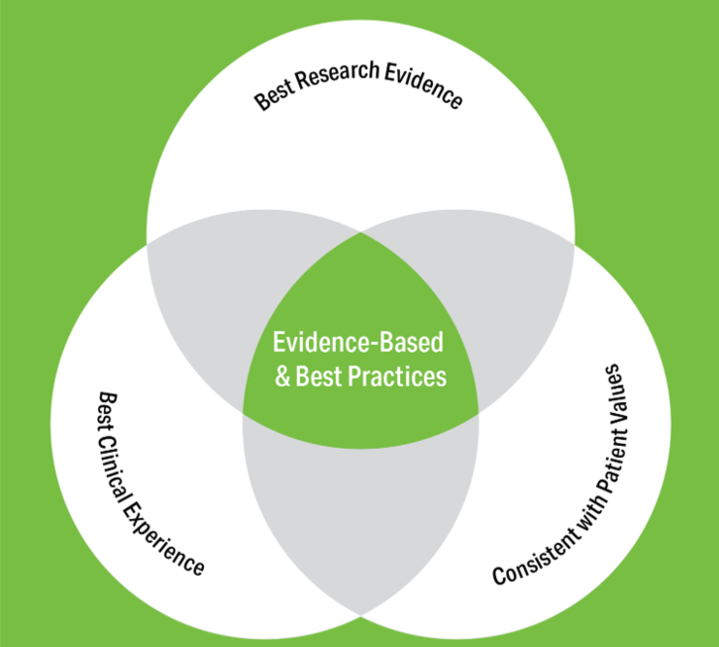
Definition of Evidence-Based Medicine
“Evidence based medicine is the conscientious, explicit, and judicious use of current best evidence in making decisions about the care of individual patients. The practice of evidence-based medicine means integrating individual clinical expertise with the best available external clinical evidence from systematic research.”
–David Sackett, MD
Sackett DL et al. Evidence-Based Medicine: How to Practice and Teach EBM. 2nd ed. Churchill Livingstone; 2000.
|
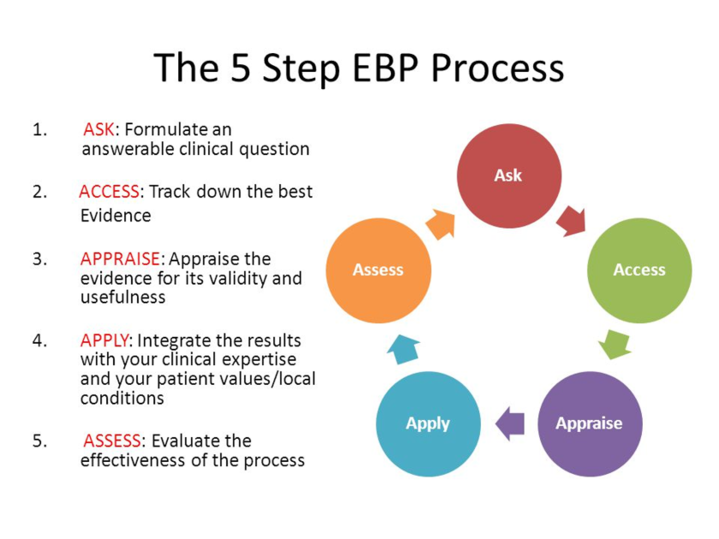
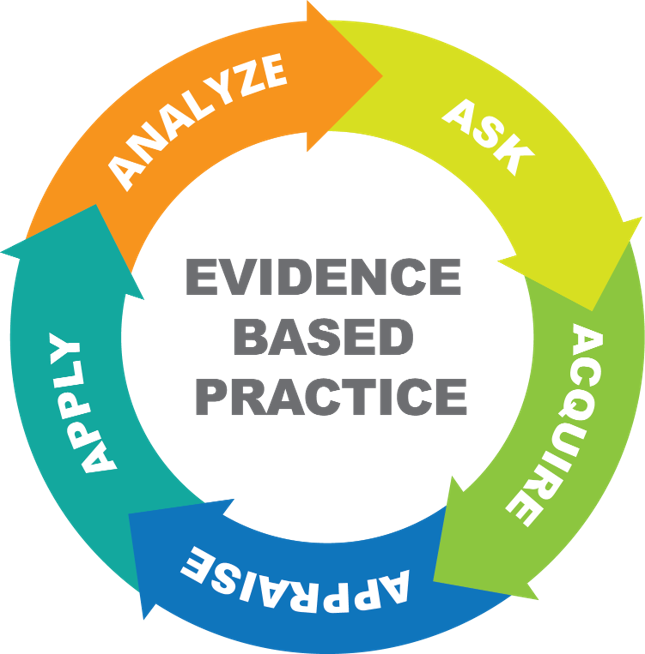
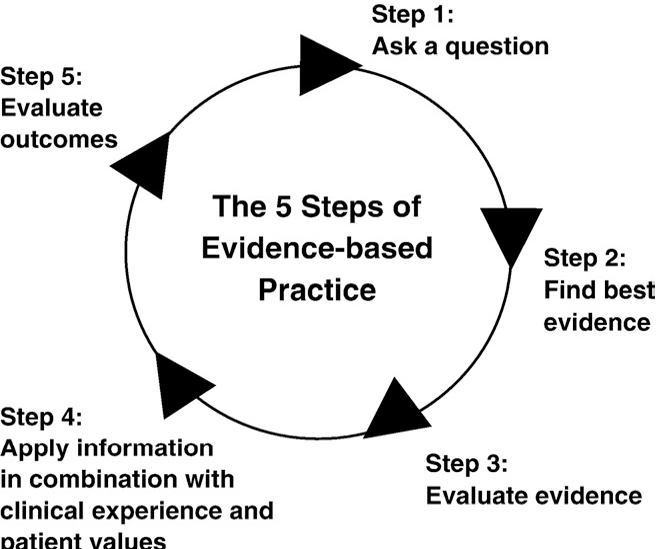
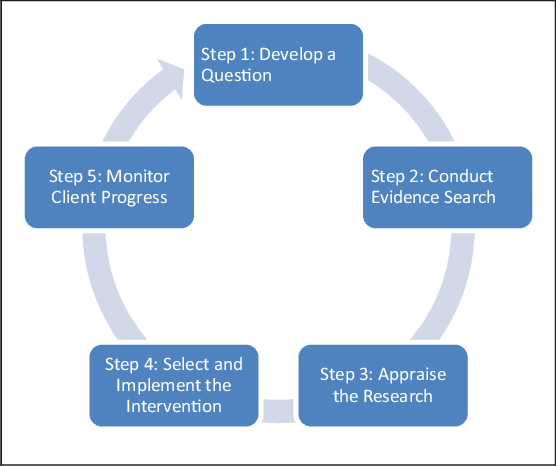
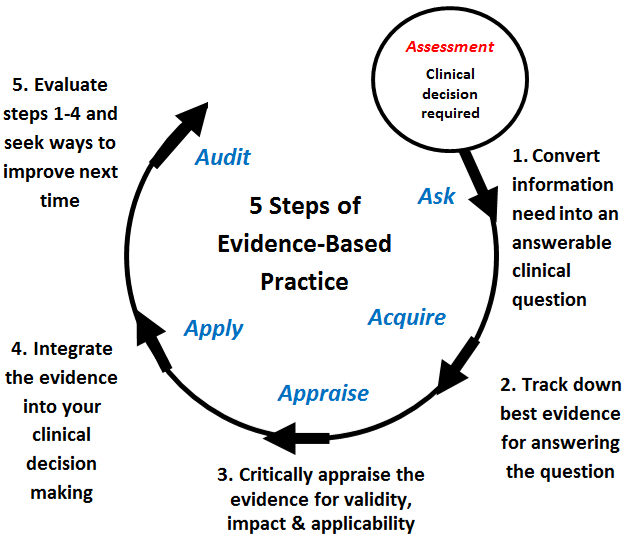
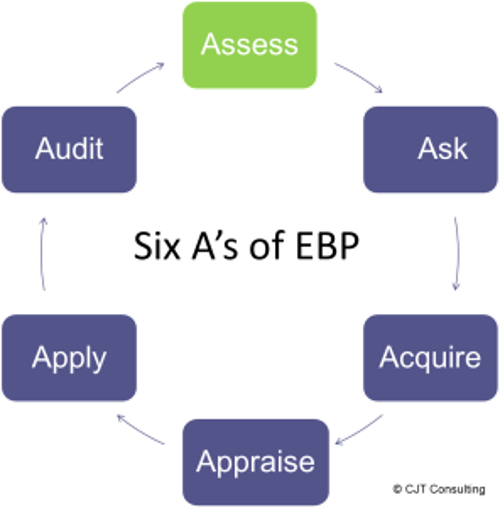
Steps in Practicing Evidence-Based Medicine
Step 1: Construct well-built and answerable clinical questions
Step 2: Locate the best evidence to answer these questions
Step 3: Critically appraise your findings
Step 4: Integrate findings with clinical expertise and patient needs
Step 5: Evaluate your performance of these steps and seek ways to improve
Sackett DL et al. Evidence-Based Medicine: How to Practice and Teach EBM. 2nd ed. Churchill Livingstone; 2000.
|
Step 1: Construct Well-Built Clinical Questions
“Background” questions
– Ask for general knowledge about a disorder
“Foreground” questions
– Ask for specific knowledge about managing patients with a disorder
Step 2: Locate the Best Evidence
Sources of information and evidence may include:
- Colleagues
- Textbooks
- Journals (e.g., evidence-based)
- Systematic reviews
- Guidelines and Electronic databases
Where to start searching may depend on:
- Available time
- Available databases
- Foreground versus background knowledge required
Step 3: Select Electronic Health Information Resources
Sackett DL et al. Evidence-Based Medicine: How to Practice and Teach EBM. 2nd ed. Churchill Livingstone; 2000.
|
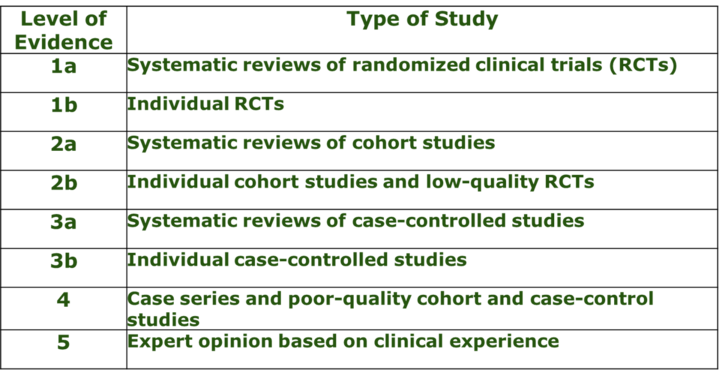
Step 5: Meta-analytic studies of Cohort RTC’s are widely accepted in the Mental Health Field
Researchers have widely accepted that meta-analytic studies support a more nuanced view of treatment efficacy because they review a number of empirically supported treatment (EST) research efforts which have used random controlled studies (RTC’s) and enables the identification of the validated and empirically supported evidence for their treatment effectiveness (Westin, Novotny and Thompson, 2004).
|
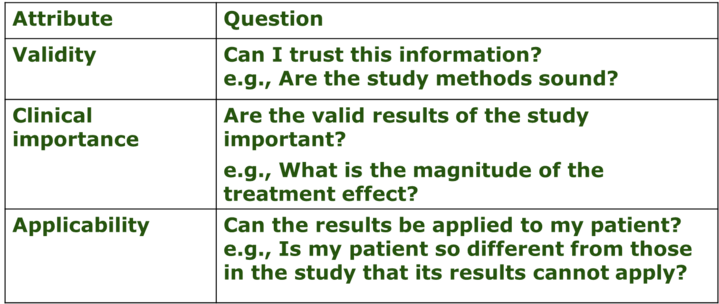
Step 6: Critically
Appraise the Evidence
|
Step 7: Integrate Findings With Clinical Expertise and Patient Needs
Critical Appraisal Patient
Clinical Decision
Clinical Expertise
|
Step 8 Evaluate Performance and Seek Ways to Improve
1.Am I asking well-formulated clinical questions?
2.Am I searching at all?
3.Do I know the best sources of current external evidence?
4.Am I critically appraising external evidence?
5.Am I integrating my critical appraisal into my practice?
|
Ongoing Evaluation of the Success of use of the EBP’s is extremely Important
- Barlow (2007) cautions that clinicians must be careful how they view using EBP’s in their clinical practice.
- They need to avoid blindly using a treatment manual and rather mindlessly administering the procedures in a rote manner.
- Barlow (2007) went on to advocate that clinicians integrate EBP’s into the treatment process based on individual client needs.
- This is exactly what the Medical Model of Evidence Based Medicine recommends
|
What does Effectiveness Mean?
The reality is that EBP’s have been effective, but have not always been universally effective, given the variety of client circumstances.
- Efficacy is the systematic scientific evaluation if a treatment is successful in lessening symptoms and mental health disorders.
- Efficacy studies use controlled studies which are not always generalizable to the real clinical world.
- Effectiveness, however, is concerned with whether an EBP works in less controlled, natural settings with all of its unpredictable variables.
- EBP’s might work in controlled studies in laboratory like settings, but are they effective in the natural mental health communities in which Mental Health Professionals work?
- Mental Health Professionals must always be aware that when selecting EBPs they must monitor the client’s response, their own personal response in executing the EBP plan and how the EBP affects or supports the therapeutic relationship between their clients and themselves.
- Mental Health Professionals need to be ready and open to adjust their treatment plans and adapt their treatment protocols to the needs, personality and make up of their specific clients to ensure their treatment goals are not undermined by too strict an adherence to the EBP protocols.
|
What are the 3 over-riding characteristics of Mental Health EBP’s?
Evidence Based Practices use three concepts:
1.Empirically supported treatments (EST) which identify specific psychotherapeutic interventions with evidence for their effectiveness in treating certain diagnoses or identified problems successfully
2.Clinical Practice Guidelines which entail assessment and treatment strategies with a recommended course of application
3.Evidence Based Practice which is a series of activities that would enable mental health practitioners to administer the best care possible to their clients or client groups under their care (Barlow, 2007).
Researchers have widely accepted that meta-analytic studies support a more nuanced view of treatment efficacy because they review a number of empirically supported treatment (EST) research efforts which have used random controlled studies (RTCs) and enables the identification of the validated and empirically supported evidence for their treatment effectiveness (Westin, Novotny and Thompson, 2004).
|
Behavioral Health Consultants need to be up on EBP’s to be effective members of an Integrated Medical Team
Behavioral Health Consultants in Integrated Medical settings, need to understand and be able to fully implement:
1.EBP oriented Clinical Assessment and Treatment Planning; Treatment Progress Notes and Case Study Format
2.Evidence Based Practices treatments for patients’ mental health disorders
3.Specific Evidence Based treatments for specific mental health disorders for each patient seen within the integrated medical settings.
|
Benefits of using EBP’s with Clients in Integrated Medical Settings
1.Benefits Patients: when the clinician informs them that the established treatment plan for their care is based on empirically supported treatment the patients gain confidence that they will receive some clinical benefit.
2.Motivates Patients: Since they need to be motivated for treatment by informing them that they will receive a “proven” treatment model helps raise their expectations for successful outcomes. It also helps to motivate them to give such treatment approaches a chance.
3.Overcomes resistance to treatment: This is a major obstacle which Behavior Health Consultants face in working with patients so anything they can do to increase patients’ motivation and participation in the treatment is most welcomed.
|
Use of EBP’s increase trust between Behavior Health Consultants and their patients
1. Accountability: When Behavioral Health Consultants choose researched treatments that have demonstrated clinical benefits, this demonstrates a sense of accountability to their patients
2. Professionalism: Using EBPs also demonstrates a professionalism and ethical soundness in their approach to treatment planning since they review the latest research and findings so as to identify appropriate interventions with some promise for success with their patients.
3. Improved Plans of Treatment: Using EBPs enables Behavioral Health Consultants to better provide a consistent rational plan of action which they can easily monitor for its implementation, management and results. This gives Behavioral Health Consultants more flexibility to alter their treatment plans since EBPs offer a variety of optional interventional approaches to achieve the same clinical treatment goals.
|
Use of EBP’s show Medical Teams that The Behavioral Health Consultants are Effective
An added goal supporting the use of EBP’s involves the opinion of other medical and mental health professions of Behavioral Health Consultants since it demonstrates to both the medical and mental health community that Behavioral Health Consultants work hard to be as effective as possible through their use of scientifically supported treatment interventions.
|
Reluctance by Professional Counseling Training Programs to embrace EBP’s
Rationale for not embracing EBP’s by Counselor Education Programs:
1.There has been a long-held belief within the mental health training establishment that Counseling is “developmental in nature with a primary focus on wellness”
2.That professional counselors should not handle diagnosing and treating major mental health disorders
3.Most importantly, the training establishment has been unwilling to embrace EBP’s given that it appears to them that EBP’s are simply “cookbook-like” manualized treatment approaches which give no freedom or latitude to the professional counselor.
Unfortunately, for this reason, all too few textbooks in professional mental health counseling have focused on EBP’s so that Clinical Mental Health Counselors in training can learn about and then put into practice these sound researched clinical interventions.
|
Reluctance in use of EBP’s in the broader Mental Health Field has been there
Even though the use of evidence-based practices has been the norm since the start of 2000, there has been real resistance to their use by clinicians. Foa, Gillihan and Bryant (2013), posited that there are many factors which explain the non-use of Evidence Based Treatments:
1.“A professional culture” that does not support the use of EBP’s
2.Lack of clinician training in EBP’s
3.limited effectiveness of commonly used dissemination techniques, and the cost associated with effective dissemination models” (Foa, Gillihan & Bryant, 2013, p. 79). These authors went on to say that: “One shared assumption in traditional psychotherapy is that understanding the origins of one’s problems and symptoms, such as difficult childhood relationships with parents, is essential for successful therapy outcome. Thus, psychotherapy is seen as an intricate process of collaboration between the patient and the therapist, whose goal is to maximize well-being and happiness by exploring multiple aspects of the patient’s inner life and experiences and helping the patient increase insight and self-understanding” (Foa, Gillihan & Bryant, 2013, p. 80).
|
Accepted Rationale for Use of EBP’s
Evidence based practices are psychological and psychotherapeutic treatments and interventions of physical and psychological pathology (Barlow, 2004).
Evidence Based Practices use three concepts:
1. Empirically supported treatments (EST) which identify specific psychotherapeutic interventions with evidence for their effectiveness in treating certain diagnoses or identified problems successfully
2. Clinical Practice Guidelines which entail assessment and treatment strategies with a recommended course of application
3.Evidence Based Practice which is a series of activities that would comprise evidenced based practices which enable mental health practitioners to administer the best care possible to their clients or client groups under their care (Barlow, 2007).
|
What are the common Mental Health disorders treated within Integrated Medical teams?
1. Autistic Spectrum Disorder
2. Attention Deficit Hyperactivity Disorder (ADHD)
3. Bipolar Disorder
4. Depressive Disorders
5. Anxiety and Trauma and Stressor-Related Disorders
6. Phobias
7. Post Traumatic Stress Disorder (PTSD)
8. Obsessive Compulsive Disorder (OCD)
9. Anorexia
10. Bulimia
11. Alcohol use Disorders
12. Substance and Medication use Disorders
|
Initial Mental Health Assessment
Date of Assessment:
Name of Client:
Chronological Age:
Date of Birth of Client:
Educational Level:
Ethnic Origin or Race:
Referred by:
Marital Status:
Why now?
Clinical Mental Health History
Current psychotropic medications.
Medical History
Family History.
Social History
Vocational History:
Client’s strengths & Liabilities
Relevant ACE (Adverse Childhood Experiences)
- Abuse: 1. Emotional Abuse 2. Physical Abuse 3. Sexual Abuse
- Neglect: 4. Emotional Neglect 5. Physical Neglect
- Household Dysfunction: 6. Mother was treated violently 7. Household substance abuse 8. Household mental illness 9. Parental separation or divorce 10. Incarcerated household member
Mental Status Exam: Appearance Consciousness Orientation Speech Affect Mood Concentration Activity Level Thoughts Memory Judgment
Tentative Diagnosis
A. Principal Diagnosis
B. Provisional Diagnosis
C. Other Conditions That May Be a Focus of Clinical Attention
Treatment Plan –
3 long term goals,
3 objectives per goal,
1 intervention per objective (Use Jungsma Planners)
|
Evidence Based Practices for Behavioral Health Consultants
To help Behavioral Health Consultants identify recognized tools for EBP’s they can use the online book: Messina, J.J. (2016), Evidence Based Practices for Mental Health Professionals. Retrieved at: http://coping.us/evidencebasedpractices.html
In this book they will be provided for the 12 Diagnoses Covered the following
1.Case Studies
2.ICD-10-CM Codes
3.DSM-5 Clinical descriptors
4.EBP’s for each of the 12 Disorders
5.Homework and handouts
6.EBP workbooks, manuals and guidebooks
7.References for EBP’s
|
Autism – Evidence Based Practices
1.Operational definition of the observed target’s undesirable behaviors such as repetitive behaviors
2.Identification of the triggers for the unwanted behaviors and development of the treatment environment which controls or eliminate such triggers
3.Task analysis which clearly explains the involved treatment procedures
4.Measurement which quantifies acquisition, maintenance and generalizes the targeted behaviors
The behavioral-psychoeducational models include
1.Classroom program called TEACCH
2.Applied Behavioral Analysis/Discrete Trial Training
3.Pivotal Response Training
4.Incidental Teaching
|
ADHD - Evidence Based Practices
Combination of medication and behavioral intervention
Clinicians have found that the combination treatment of medication and behavioral intervention are most successful in addressing the ADHD symptomatology
|
Bipolar Disorder – Evidence Based Practice
The use of pharmacotherapy is a major EBP in treating Bipolar Disorder
Note: Unfortunately, clients are typically non-compliant in taking their medications as directed.
All too often these clients are “set up” to expect improvement and have no idea that they are coping with a chronic condition
Cognitive Behavioral Therapy is an adjunctive therapy which helps patients better understand:
- the extreme mood swings
- their beliefs which lead to non-compliance
- distressing intrusive memories which can be derailing
- irrational thinking which keeps them stuck or unwilling to work on overcoming the impact of their disorder
|
Depression – Evidence Based Practices
1.Pharmacotherapy only
2.Cognitive Behavioral Therapy (CBT) only
3.Combination of CBT with other therapies: a) Positive Psychology b) Mindfulness c) Acceptance and commitment therapy
4.Interpersonal Psychotherapy (IPT)
5.Process-Experiential Therapy (PET)
6.Combination of medication and individual therapy
7.Exercise with older adults
8.Family therapy or psychoeducation
|
Anxiety – Evidence Based Practices
1.Pharmacological Treatments only
2.Psychotherapeutic interventions only
- 1. Cognitive Behavioral Therapy or
- 2. Behavioral Exposure Treatments
3. Combination of CBT and medications
|
Phobias – Evidence Based Practices
1.Cognitive Behavioral Therapy (CBT)
2.In vivo Exposure
3.Virtual Exposure
4.Combination of CBT and Exposure
5.Eye Movement Desensitization and Reprocessing (EMDR)
6.Pharmacotherapy only
|
PSTD – Other Trauma Related Conditions – Evidence Based Practices
1. Trauma Focused Cognitive Behavioral Therapy (FTCBT) or Cognitive Processing Therapy (CPT)
2. Prolonged Exposure (PE)
3. Eye Movement Desensitization and Reprocessing (EMDR)
4. Pharmacotherapy
|
Obsessive-Compulsive Disorder – Evidence Based Practices
1.Cognitive Behavioral Therapy (CBT) or Cognitive Therapy (CT)
2.Exposure and Response Prevention (ERP)
3.Pharmacotherapy
4.Combination CBT/CT or ERP and Pharmacotherapy
|
Anorexia – Evidence Based Practices
1.Cognitive Behavior Therapy or Behavioral Therapy
2.Inpatient/outpatient treatment program for weight restoration with combination of CBT, medication and weight restoration and nutritional counseling and psychoeducation
Bulimia - Evidence Based Practices
1.Psychological Treatment only: Cognitive Behavior Therapy (CBT) or Interpersonal Psychotherapy (IPT)
2.Family Therapy included in Outpatient Program
3.Group Therapy included/or alone in Outpatient Program
4.Technology: Internet based CBT individual treatment
5.Self-Help Programs
6.Pharmacotherapy only
7.Combination of Psychological and Pharmacotherapy
|
Alcohol Use Disorder – Evidence Based Practices
1. AA only
2.Cognitive Behavior Therapy (CBT)
3.Motivational Interviewing only
4.CBT and Motivational Interviewing
5.Family or Couples Therapy (Walitzer and Dermen, 2004; Harris, Baker, Kimball and Shumway, 2007, Deas, 2008).
6.Residential or outpatient with combination of CBT and AA
7.AA as aftercare for either Residential or Outpatient Treatment
8.Internet/Virtual Reality
9.Pharmacotherapy only
|
Substance Use Disorder – Evidence Based Practices
1. Cognitive behavior therapy (CBT)
2. Motivational Interviewing (MI)
3. Contingency Management (CM)
4. Supportive-Expressive (SE) Psychotherapy
5. Multisystemic (Family) Therapy (MST)
6. Pharmacotherapy only
7.12 Step Programming
8. Computer and Technology Supported
|
References
Barlow, D.H. (2005). Clarification on psychological treatments and psychotherapy. American Psychologist, 60(7), 734-735. doi: 10.1037/0003-066X.60.7.
Barlow, D.H. (2010). Negative effects from psychological treatments. American Psychologist, 65(1), 13-20. doi: 10.1037/a0015643
Barlow, D. H. (2004). Psychological treatments. American Psychologist, 59(9), 869-878. doi: 10.1037/0003-066X.59.9.869
Barlow, D, H. (2006). Psychotherapy and psychological treatments: The future. Clinical Psychology: Science and Practice, 13(3), 216-220. doi: 10.1111/j.1468-2850.2006.00027.x
Barlow, D. (2007). The case of hope: Evidenced based practice (EBT) in action. Pragmatic Case Studies in Psychotherapy, 3(4), 50-62.
Foa, E.B., Gillihan, S.J. & Bryant, R.A. (2013). Challenges and success in dissemination of evidenced-based treatments for posttraumatic stress: Lessons learned from prolonged exposure therapy for PTSD. Psychological Science in the Public Interest, 14(2), 65-111. DOI: 10.1177/1529100612468841
McHugh, R.K. and Barlow, D.H. (2010). The dissemination and implementation of evidenced-based psychological treatments. American Psychologist, 65(2) 73-84, doi: 10.1037/a0018121
Messina, J.J. (2016). Evidence based practices for mental health professionals. Retrieved at: http://coping.us/evidencebasedpractices.html
Sackett DL et al. (2000). Evidence-Based medicine: How to practice and teach EBM. 2nd ed. Churchill Livingstone
Westen, D., Novotny, C. and Thompson-Brenner, H. (2004). The empirical status of empirically supported psychotherapies: Assumptions, findings, and reporting in controlled clinical Trials. Psychological Bulletin, 130(4), 631-883. DOI: 10.1037/0033-2909.130.4.631
|
|
|