Co-Occurring Substance Use
& Mental Health Disorders
|
|
Treatment for Alcohol & Substance Use Disorders A Training Resource
By Jim Messina, Ph.D., CCMHC, NCC, DCMHS-T
|
|
|
Co-Occurring Disorders of Substance Use & Mental Health Disorders
CEU’s: 3 hours based on request (CE Broker Tracking #: 20-615480)
Resource for Course on Coping.us:
http://www.coping.us/alcoholsubstanceuse/comorbiddisorders.html
Program Description: This program is focused on the co-occurring mental health disorders which can be co-morbid with substance use disorders according to the DSM-5 including: Schizophrenia, Bipolar Disorder, Depression, Anxiety, Obsessive Compulsive Disorder, Sleep-Wake Disorders, Sexual Dysfunctions and Neurocognitive Disorders by the specific substances which have been identified as co-occurring with the specific mental health disorders. There is a need for therapists to understand the brain and neurological functions which lie as the cause of these co-morbidities. There is a need to treat co-occurring disorders in an integrated fashion and not rely on "old school" models of treating them sequentially, parallel separately or left untreated. To help bring home the application of co-morbid interventions case studies will be used widely in this workshop.
Learning Objectives
1.To learn about the tools to assess and Apps to treat these co-morbidities.
2. To learn about the neurological functions in the brain which lie as the cause of these co-morbidities.
3. To learn the rationale behind the need to use integrated treatment strategies when addressing these co-morbidities.
4. To learn about why it is impossible to just treat one condition in isolation from the other co-morbidities if one wants to gain maximal effectiveness for the patients suffering from them.
|
DSM-5's ICD-10-CM Codes for Substance Use Disorders
Specifiers which apply to these disorders where indicated:
- Specify if: In early remission or in sustained remission
- Specify if: In a controlled environment
- Specify if: With perceptual disturbances
Alcohol-Related Disorders
F10.10 Alcohol Use Disorder Mild
F10.20 Alcohol Use Disorder Moderate
F10.20 Alcohol Use Disorder Severe
F10.129 Alcohol Intoxication With use disorder Mild
F10.229 Alcohol Intoxication With use disorder Moderate or severe
F10.929 Alcohol Intoxication Without use disorder
F10.239 Alcohol Withdrawal Without perceptual disturbances
F10.232 Alcohol Withdrawal With perceptual disturbances
F10.99 Unspecified Alcohol-Related Disorder
Cannabis-Related Disorders
F12.10 Cannabis Use Disorder Mild
F12.20 Cannabis Use Disorder Moderate
F12.20 Cannabis Use Disorder Severe
F12.129 Cannabis Intoxication Without perceptual disturbance with use disorder Mild
F10.229 Cannabis Intoxication Without perceptual disturbance With use disorder Moderate or severe
F10.929 Cannabis Intoxication Without perceptual disturbance Without use disorder
F12.122 Cannabis Intoxication With perceptual disturbance with use disorder Mild
F10.222 Cannabis Intoxication With perceptual disturbance With use disorder Moderate or severe F10.922 Cannabis Intoxication With perceptual disturbance Without use disorder
F12.288 Cannabis Withdrawal
F12.99 Unspecified Cannabis-Related Disorders
|
Hallucinogen- Related Disorders
Hallucinogens:
- Indole Alkaloids: ( Lysergic acid diethylamide (LSD); Lysergic acid amide (LSA); Psilocin; Psilocybin)
- Pipendines: (Atropine and scopolamine); Cocaine; Phencyclidine (PCP); Ketamine)
Phenylethylamines:
- (Mescaline, 3,4- methylenedioxymethamphetamine (MDMA), Methylene dioxyamphetamine (MDA), 3-methoxy-4, 5-methylene dioxyamphetamine (MMDA), 3,5-dimethoxy-4-methylamphetamine (STP), 2,5-dimethoxy-4-methylamphetamine (DOM))
Cannabinoids:
- (Delta-9-tetrahydrocannabinol (THC, the active substance in marijuana)
F16.10 Phencyclidine Use Disorder Mild
F16.20 Phencyclidine Use Disorder Moderate
F16.20 Phencyclidine Use Disorder Severe
F16.10 Other Hallucinogen Use Disorder Mild
F16.20 Other Hallucinogen Use Disorder Moderate
F16.20 Other Hallucinogen Use Disorder Severe
F16.129 Phencyclidine Intoxication With use disorder Mild
F16.229 Phencyclidine Intoxication With use disorder Moderate or severe
F16.929 Phencyclidine Intoxication Without use disorder
F16.129 Other Hallucinogen Intoxication With use disorder Mild
F16.229 Other Hallucinogen Intoxication With use disorder Moderate or severe
F16.929 Other Hallucinogen Intoxication Without use disorder
F16.983 Hallucinogen Persisting Perception Disorder
F16.99 Unspecified Phencyclidine-Related Disorder
F16.99 Unspecified Hallucinogen-Related Disorder
|
Inhalant-Related Disorders
Specify the particular inhalant
Mood-altering substances that are voluntarily inhaled
- Butyl nitrite
- Amyl nitrite (Gas in aerosol cans),
- Gasoline and Toluene vapors (Correction fluid, glue, marking pens)
- Most substances used are commercial and household products, such as solvents and aerosols, which are easily obtained and typically not harmful, if used for the purpose intended and as directed
- Because they are common products, inhalants often are a young person’s first attempt at “getting high”
F18.10 Inhalant Use Disorder Mild
F18.20 Inhalant Use Disorder Moderate
F18.20 Inhalant Use Disorder Severe
F18.129 Inhalant Intoxication With use disorder Mild
F18.229 Inhalant Intoxication With use disorder Moderate or severe
F18.929 Inhalant Intoxication Without use disorder
F18.99 Unspecified Inhalant-Related Disorders
|
Opioid-Related Disorders
Opioides:
- Morphine
- Morphine long-acting (Avinza, Kadian)
- HYDROmorphone (Dilaudid)
- OXYcodone (Oxecta): OXYcodone, long-acting (OxyContin)
- HYDROcododone (Vicodin, Lortab) OXYmorphone (Opana)
- OXYmorphone, long-acting (Opana ER)
- Codeine
- Fentanyl
- Methadone
Specify if: on maintenance therapy or in a controlled environment
F11.10 Opioid Use Disorder Mild
F11.20 Opioid Use Disorder Moderate
F11.20 Opioid Use Disorder Severe
F11.129 Opioid Intoxication Without perceptual disturbance with use disorder Mild
F11.229 Opioid Intoxication Without perceptual disturbance With use disorder Moderate or severe
F11.929 Opioid Intoxication Without perceptual disturbance Without use disorder
F11.122 Opioid Intoxication With perceptual disturbance with use disorder Mild
F11.222 Opioid Intoxication With perceptual disturbance With use disorder Moderate or severe
F11.922 Opioid Intoxication With perceptual disturbance Without use disorder
F11.23 Opioid Withdrawal
F11.99 Unspecified Opioid -Related Disorders
|
Sedative-, Hypnotic-, or Anxiolytic-Related Disorders
Sedatives:
Barbiturates:
- Methohexital (Brevital) and thiopental (Pentothal);
- Amobarbital (Amytal), pentobarbital (Nembutal), secobarbital (Seconal), and butalbital (Fioricet, Fiorinal);
- Phenobarbital (Luminal)
Non-Barbiturates:
- Benzodiazepines: Carbamates - Meprobamate (Miltown)
- Chloral derivatives - Chloral hydrate (Noctec) and Ethchlorvynol (Placidyl)
- Piperidines - Glutethimide (Doriden) and methyprylon (Noludar)
- Quinazolinone - Methaqualone (Quaalude)
- Imidazopyridine - Zolpidem (Ambien), zaleplon (Sonata), eszopiclone (Lunesta) and alpidem
- Antihistamines (over-the-counter sleep aids) - Diphenhydramine and doxylamine
- GHB- Gamma-hydroxybutyrate
Hypnotics:
Benzodiazepines:
- Diazepam (Valium, Diastat; Diastat AcuDial)
- Lorazepam (Ativan)
- Midazolam(Versed)
Anxiolytics (Anti-anxiety Meds):
- Alprazolam (Xanax, Niravam, Xanax XR)
- Lorazepam (Ativan)
- Chlordiazepoxide (Librium)
- Clonazepam (Klonopin)
- Clorazepate (Tranxene SD; Tranxene T-Tab)
- Diazepam (Valium, Diastat; Diastat AcuDial)
- Midazolam (Versed)
- Oxazepam (Serax)
F13.10 Sedative, Hypnotic, or Anxiolytic Use Disorder Mild
F13.20 Sedative, Hypnotic, or Anxiolytic Use Disorder Moderate
F13.20 Sedative, Hypnotic, or Anxiolytic Use Disorder Severe
F13.129 Sedative, Hypnotic, or Anxiolytic Intoxication with use disorder Mild
F13.229 Sedative, Hypnotic, or Anxiolytic Intoxication with use disorder Moderate or severe
F13.929 Sedative, Hypnotic, or Anxiolytic Intoxication without use disorder
F13.239 Sedative, Hypnotic, or Anxiolytic Withdrawal Without perceptual disturbance
F13.222 Sedative, Hypnotic, or Anxiolytic Withdrawal With perceptual disturbance
F13.99 Unspecified Sedative-, Hypnotic-, or Anxiolytic- Related Disorder
|
Stimulant-Related Disorder
Amphetamine Related:
F15.10 Amphetamine-Type Substance Use Disorder Mild
F15.20 Amphetamine-Type Substance Use Disorder Moderate
F15.20 Amphetamine-Type Substance Use Disorder Severe
F15.129 Amphetamine or other stimulant Intoxication Without perceptual disturbance with use disorder Mild
F15.229 Amphetamine or other stimulant Intoxication Without perceptual disturbance With use disorder Moderate or severe
F15.929 Amphetamine or other stimulant Intoxication Without perceptual disturbance Without use disorder
F15.122 Amphetamine or other stimulant Intoxication With perceptual disturbance with use disorder Mild
F15.222 Amphetamine or other stimulant Intoxication With perceptual disturbance With use disorder Moderate or severe
F15.922 Amphetamine or other stimulant Intoxication With perceptual disturbance Without use disorder
F15.23 Amphetamine or other substance Withdrawal
F15.99 Unspecified Amphetamine or other substance-Related Disorders
Cocaine Related:
F15.10 Cocaine Use Disorder Mild
F15.20 Cocaine Use Disorder Moderate
F15.20 Cocaine Use Disorder Severe
F14.129 Cocaine Intoxication Without perceptual disturbance with use disorder Mild
F14.229 Cocaine Intoxication Without perceptual disturbance With use disorder Moderate or severe
F14.929 Cocaine Intoxication Without perceptual disturbance Without use disorder
F14.122 Cocaine Intoxication With perceptual disturbance with use disorder Mild
F14.222 Cocaine Intoxication With perceptual disturbance With use disorder Moderate or severe
F15.922 Cocaine Intoxication With perceptual disturbance Without use disorder
F14.23 Cocaine Withdrawal
F14.99 Unspecified Cocaine-Related Disorders
Other or Unspecified Stimulant:
F15.10 Other or unspecified stimulant Use Disorder Mild
F15.20 Other or unspecified stimulant Use Disorder Moderate
F15.20 Other or unspecified stimulant Use Disorder Severe
|
Other (or unknown) Substance-Related Disorders
F19.10 Other (or unknown) Substance Use Disorder Mild
F19.20 Other (or unknown) Substance Use Disorder Moderate
F19.20 Other (or unknown) Substance Use Disorder Severe
F19.129 Other (or unknown) Substance Intoxication With use disorder Mild
F19.229 Other (or unknown) Substance Intoxication With use disorder Moderate or severe
F19.929 Other (or unknown) Substance Intoxication Without use disorder
F19.239 Other (or unknown) Substance
F19.99 Unspecified Other (or unknown) Substance -Related Disorder
|
Co-occurring Substance Use Disorders & Mental Health Disorder Treatment Focus
Substance /Medication – Induced Disorders
- Schizophrenia
- Bipolar Disorder
- Depressive Disorders
- Anxiety Disorders
- Obsessive Compulsive Disorder
- Sleep-Wake Disorders
- Sexual Dysfunctions
- Neurocognitive Disorders
|
What follows are the Classifications for co-occuring Substance use Disorder and Mental Health Disorders
Co-occurring Substance Disorder with Schizophrenic Induced Psychotic Disorder
- Alcohol
- Cannabis
- Phencyclidine
- Hallucinogens
- Inhalants
- Sedatives
- Amphetamines
- Cocaine
Co-occurring Substance Disorder with Bipolar & Related Disorders
- Alcohol
- Phencyclidine
- Hallucinogens
- Sedatives
- Amphetamines
- Cocaine
Co-occurring Substance Disorder with Depressive Disorders
- Alcohol
- Phencyclidine
- Hallucinogens
- Inhalants
- Opioid
- Sedatives
- Amphetamines
- Cocaine
Co-occurring Substance Disorder with Anxiety Disorders
- Alcohol
- Caffeine
- Cannabis
- Phencyclidine
- Hallucinogens
- Inhalant
- Opioid
- Sedative
- Amphetamine
- Cocaine
Co-occurring Substance Disorder with Obsessive-Compulsive Disorder
Co-occurring Substance Disorder with Sleep-Wake Disorders
- Alcohol
- Caffeine
- Cannabis
- Sedative
- Amphetamine
- Cocaine
- Tobacco
Co-occurring Substance Disorder with Sexual Dysfunctions
- Alcohol
- Opioid
- Sedative
- Amphetamine
- Cocaine
Co-occurring Substance Disorder with Delirium & Neurocognitive Disorders
- Alcohol
- Cannabis
- Phencyclidine
- Hallucinogens
- Inhalant
- Opioid
- Sedative
- Amphetamine
- Cocaine
|
Likelihood of SUDs in people with psychiatric diagnoses
Diagnosis Odds Ratio*
Bipolar Disorder 6.6
Schizophrenia 4.6
Panic Disorder 2.9
Major Depression 1.9
Anxiety Disorder 1.7
*Weiss, R.D. & Smith-Connery, H. (2011). Integrated Group Therapy for Bipolar Disorder and Substance Abuse. New York: Guilford Press
|
Why Substance abuse in patients with psychiatric illness?
- Enhanced reinforcement
- Mood Change
- Escape
- Hopelessness
- Poor Judgment
- Inability to appreciate consequences
Results of SUD with Psychiatric Disorder especially Bipolar Disorder
- Lower medication adherence
- Greater chance relapses
- Increased hospitalizations
- Homelessness
- Suicide
Models of Treatment for Dual Diagnosis
- Sequential – Treat SUD first then Psychiatric disorder
- Parallel – Treat both at same time but within different treatment modalities
- Integrated – Treat both at same time within the same treatment modality
Integrated Treatment Model of Treatment of Comorbid Disorders
- Cognitive‐behavioral model focuses on parallels between the disorders in recovery/relapse thoughts and behaviors
- Explores the interaction between the two disorders
- Utilizes a single disorder paradigm: “bipolar substance abuse”
- Uses a “Central Recovery Rule”
Focus of Integrated Model
- Dealing with the Psychiatric disorder without use of Alcohol &/or Drugs
- Confronting denial, ambivalence, acceptance
- Monitoring overall mood during each week
- Emphasis on compliance in taking psychiatric medications
- Identifying and fighting triggers
- Emphasis on “wellness” model of good night’s sleep, balance nutritional intake and exercise
Parallels in Recovery & Relapse thinking between Disorders
- “May as well thinking” vs. “It matters what you do”
- Abstinence violation effect vs. stopping taking psychiatric meds when anxious or depressed
- Recovery thinking vs. relapse thinking and acting out
- Remember: you’re always on the road to getting better or getting worse: “It matters what you do!”
The Central Recovery Rule
No matter what
- Don’t drink
- Don’t use drugs
- Take your medication as prescribed
No matter what
Weiss, R.D. & Smith-Connery, H. (2011). Integrated Group Therapy for Bipolar Disorder and Substance Abuse. New York: Guilford Press.
|
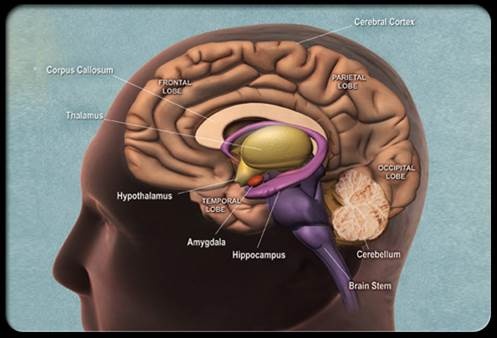
Neuroscience Look at Substance Use Disorders
Frontal (Executive) Cortical Function
- Focus attention
- Prioritize
- Exclude extraneous information
- Suppress primitive urges
- Reduce impulsivity
Non-Addict Response
“This is dangerous”
Prefrontal cortex
- Sends inhibitory signals to the Ventral Tegmental Area (VTA)
- Reduces dopamine release
No repetitive use pattern
No reinforcement of pleasure
Addict Response Pattern
“Got to have more”
Cognitive Deficit Model
Abnormalities in prefrontal cortex
- Compromised ability to send inhibitory signal to VTA
- Chronic alcoholics have reduced GABA
Neurochemical used in the inhibitory process
- Meth and Coke may damage this brain loop
- Frontostriatal loop
|
Driving Forces of Addictive Disorder
- Acute Abstinence Syndrome
- Situational and emotional triggers
- Reward and reinforcement
Tolerance
Brain cells gradually become less responsive
- More is needed to stimulate the VTA brain cells
- To cause more release of dopamine in the NAc
- To produce reward comparable to earlier experiences
Acute Abstinence Syndrome (Heroin)
Locus Coeruleus (LC)
Norepinephrine (NE)
- Wakefulness
- Breathing
- Blood pressure
- General Alertness
Heroin attaches to mu opioid receptors in LC
- Suppression of NE
- Drowsiness
- Slowed respiration
- Low blood pressure
Symptoms of the Abstinence Syndrome (Heroin)
Addicts experience- A hyper-aroused state(“fight or flight”) with
Increased :
- Heart rate
- Blood pressure
- Restlessness
- Tremors
- Hypervigilence
- Dilated pupils
Symptoms of the Abstinence Syndrome (Heroin)
Addicts experience-worst case of flu imaginable
- Nausea and vomiting
- Runny nose
- Cold,shivering
- Cramping
- Tearing
- Diarrhea
Multiple Interlocking Neurotransmitter Systems
Dopaminergic system
Serotonergic system
Noradrenergic system
Gamma amino butyric acid (GABA) system
Glutamatergic system
Acute Abstinence Syndrome
Mesolimbic Reward System
- Reduction of the VTA’s release of dopamine into Nucleus Accubens (NAc) resulting in Anhedonia
Changes in reward system are part of craving and compulsive drug use
Principles of Acute Management
- Long acting for short acting
- Intoxication not necessary
- 20-30% reduction will not precipitate an abstinence syndrome
- Long term slow withdrawal without patients knowledge of dosage best in outpatient
Alcohol Acute Abstinence Syndrome
- Activation of excitatory glutamatergic system which can induce-Seizures
- Inhibition of inhibitory GABA system
- Net effect is sympathetic nervous system hyperactivity
Medication Management of Alcohol Acute Abstinence Syndrome
Benzodiazepines
GABA agonists
- Attenuate GABA activity
- Reduce seizure risks
Long acting benzodiazepines
- Chlordiazepoxide (Librium)
- Diazepam (Valium)
- Clonazepam (Klonopin)
Alpha-2 Adrenergic Agonists-Reduce Norepinephrine activity
- Clonidine (Catapres)
- Lofexidine (Britlofex)
Beta-Adrenergic Blockers-Block peripheral symptoms
- Tremors
- Increased heart rate
- Sweating
- Propranolol (Inderal)
Medications To Reduce Alcohol Relapse Rate
Disulfiram (Antabuse)
- Inhibits liver enzyme aldehyde dehydrogenase
Revia (Naltrexone)
- Opioid antagonist
- Enhanced release of Beta-Endorphins with family history
Acamprosate
- Inhibits Glutamatergic activity
- Enhances GABA activity
Selective Serotonin Reuptake Inhibitors-Reduce amount of drinking in heavy drinkers
- Fluoxetine (Prozac)
- Citalopram (Celexa)
Topiramate (Topamax)
- Enhances GABA functioning
- Decreases Glutamatergic functioning
- Cognitive (concentration) problems
Situational and Emotional Triggers
Personality and change
Therapy/symptom match
Motivation
Psychotherapy
- Cognitive Therapy
- Behavior Therapy
Cognitive dysfunction and change
Education
Personality and Change
- Temperament
- Character
- Introvert vs. Extrovert
- Personality Disorder
- Cognitively open vs. closed
- Degree of impulsivity
- Stimulus seeking
Therapy/Symptom Match
Matching therapy to symptoms
- Cognitive-pessimism and self doubt, negative “self-talk”, “stinking thinking”
- Pharmacological-moderate to severe symptoms
- Interpersonal-social isolation and disturbed relationships
- Family/Couples-domestic conflict
- Insight-guilt, anger and emotional turmoil
- Behavioral-negative behaviors
- Motivational-no plans or ambivalence to change
All treatments ultimately affect all symptoms
Symptoms are related
Therapist must find a place to break into the circle
Motivation
- Motivational Interviewing
- Motivational Enhancement Therapy
- Evoking self-motivation
- Asking open-ended questions
- Stages of change model
Evoking Self-Motivation
Questions to ask
- What things make you think that this is a problem?
- What do you think will happen if you do not make a change?
- What are the reasons you see for making a change?
- What makes you think you need to make a change?
- What makes you think that if you decided to make a change, you could do it?
- What do you think would work for you, if you needed to change?
- How much does your use concern you?
Open-Ended Questions
What brings you here today?
- So you are here to talk about quitting.
In what ways are you concerned about your marijuana use?
- Do you use marijuana too much?
What do you think you want to do about your use?
- When do you plan to quit?
Stages of Change Model
- Precontemplation
- Contemplation
- Preparation
- Action
- Maintenance
Precontemplation
Task- to increase discrepancy
Educational confrontation
- How many joints do you smoke?
- Use progression models
- Accurate information about disease
- Educational model
Good and less good aspects
- Good and bad aspects
- Invites defensiveness
- Narcissistic defense
Broad based assessment
- Alcohol and drug history
- Psychosocial history
- Psychiatric evaluation
- Medical evaluation
Contemplation
Task- tip the decisional balance scale
Normalize ambivalence
- I know many other clients who felt the same way as you and they succeeded.
- You are the best judge of which way to go.
- Use reframes
What are the options?
- Move from external to internal motivation
- Real from perceived
There are many problems
- Deal with first other issue
- “Natural link”
Quit drinking for a week
Take meds for a month
List of concerns
Questions
- It’s up to you…….
- What do you plan to do next?
- What is most important reason to change?
- Where do we go from here?
- How would you like for things to turn out?
Psychotherapy
Behavior Therapy
- Understand and Change Negative Behaviors
- Positive Reinforcing Behaviors
New Social Environment
New Friends
New Activities
Based on ego-strength or level of developmental maturity
- Problem solving
- Experiential role-play
- PPT group
Contingency management
Cognitive Behavioral Therapy
Cognitive Therapy Automatic Thoughts
- “I cannot do anything right”
- “I fail at everything I do”
- “I will never get better”
- “No one can help me”
- “No one understands me”
Develop a Dynsfunctional Thought Record
Automatic Thought - Emotion - Alternative Response - Result
Cognitive Dysfunction and Change
Frontal cortex vs. midbrain
Approximately 50% entering treatment suffer from cerebral (cognitive) dysfunction
- Less likely to attend continuing care
- Less likely to be employed
- Often mistaken as resistant or unmotivated
- Less able to absorb information
Stimulant addicts look like they have degenerative brain disease
Executive and visuospatial functioning problems include:
- Recent memory
- Abstraction
- Problem solving
- Cognitive flexibility
- Planning
- Rapid Response
Recovery in neuropsychological functioning - Most of treatment is during time of greatest dysfunction
Recovery is:
- Time-dependent
- Due to sustained abstinence
- Experience-dependent
- Active rehabilitation or repetitive behavior
Education
Why give a cocaine or methamphetamine addict a 60 minute didactic or video?
A new format
- 15-20 minute simple didactic - How to participate in treatment
- 10 minute questionnaire
- 30 minute discussion group
10 Minute Questionnaire
I think...
I feel...
I learned...
My future behavior will change in this way....
Reward and Reinforcement
- Mesolimbic Reward Center
- Allostasis and Anhedonia
- Environment
- Spirituality
Mesolimbic Reward System
- Drug enters the system (heroin)
- Attaches to specialized protein - Mu opioid receptor
- Activates Ventral Tegmental Area (VTA)
- Nucleus Accumbens (NAc) releases dopamine
- Pleasure (reward)
Reward and Reinforcement
Three-way link
- Environment
- Dopamine D2 Receptor function
- Drug self-administration
Allostasis and Anhedonia
6-7 second “mental orgasm”
What’s in it for me?
Allostasis
- Inability to return to previous homeostatic levels
Anhedonia
- Inability to experience pleasure
Allostasis
- Addictive drugs dysregulate the brains reward center
- Brain stabilizes at a more negative affect state
- “Normal” becomes a more negative and unpleasant reality
- “Use just to feel normal”
Anhedonia
Attributed to a lowered level of dopamine
Cocaine and methamphetamine
Selegiline (Carbex, Atapryl)
- MAOI
- Believed to restore depleted dopamine
Modafinil (Provigil)
- Treatment for Narcolepsy
- Increases mood, energy, and sense of well-being
- Reduces daytime sleepiness
Heroin
Methadone
Clonidine
Environment
- Triggers or cues (seeing, smelling, touching, tasting, and hearing)
- that remind the addict of some aspect of his/her use
- increase the desire for the reward (craving) without necessarily enhancing the pleasure of the reward itself.
- Living in an enriched environment may reduce animals self-administration of drugs
- Animal studies suggest that environmental conditions may affect the activity of dopamine
Impact the The Environment through
Case Management
Multisystem Therapy
“Wrap around” services
- Family and childcare services
- Housing/Transportation services
- Financial and legal services
- AIDS and medical services
- Addiction and mental health services
- Vocational and educational services
|
|
|